Acute neck and nerve-root pain describes several conditions that affect the cervical spine region, and can also cause head pain. In the long term, it is rarely as disabling as low-back pain, but the severity of acute nerve-root pain ca be just as bad as sciatica.
Neck Pain
Causes of Acute Neck and Nerve Root Pain
This pain can be caused by strain of the facet joints and ligaments, and disc herniation. Muscular pain is more of a chronic condition but can flare up. Your neck is also vulnerable to extend indirect trauma, as in whiplash syndrome. When acute neck pain arises spontaneously in young adults or adolescents it is called acute torticollis, or “wry neck”. Disc prolapse with nerve-root compression is the cause of the most severe pain.
Symptoms of Acute Neck and Nerve Root Pain
You may feel sharp pain, centrally or to one side of the neck, with intense, dull aching that can spread further into the shoulder blade area and half-way down the thoracic spine. You may have stiffness due to your spine being trapped by a muscle spasm (known as “splinting”), and worse pain on certain movements such as bending forwards, backwards, sideways, or rotating. You may also find it hard to sit in a car or at a computer for long periods. The pain is often troublesome at night and lying down may make it worse. If a nerve is compressed or irritated, a sharp pain will radiate down your arm as far as your hand, accompanied by sensory disturbance such as pins and needles or numbness. If your motor nerve fibres have been damages, you may develop weakness in your upper arm/or forearm.
Risks and Complications of Acute Neck and Nerve Root Pain
The risk of serious consequences of acute neck pain is extremely small. Most of the time the pain eases over a few weeks without specific treatment The main risk lies in too much rest, the fear of triggering pain through everyday movements, and the idea that more pain means further harm, as these can lead to loss of confidence and mobility. If you have developed pain after direct trauma such as a blow to the back of the neck, then you should obtain immediate medical advice.
Treatment for Cervical Disc Herniation
Seek Medical Attention
If you suspect your pain is caused by a cervical disc herniation, you should:
Relieve your pain by finding the least painful position.
Use ice pack for the first day of pain.
Take painkillers.
Try not to rest for more than 2-3 days.
If after 7-10 days and you are still feeling pain, you should:
Stay as active and mobile as you can, while being careful to avoid extreme movements of your neck.
Avoid prolonged reaching or working with your arms extended.
See a doctor for stronger painkillers.
If after 2-4 weeks and you are still feeling pain, you should:
Consult a doctor for further examination and treatment.
See a specialist for an epidural steroid or nerve-root injection.
If after 6-8 weeks and you are still feeling pain, you should:
You may need to have an X-ray, MRI or blood test for further evaluation.
Treatment for Acute Torticollis
Seek Medical Attention
If you suspect your pain is caused by acute torticollis, you should:
Use ice packs and take some painkillers
If after 3 days and the pain increases, you should:
Avoid prolonged static positions
If after 7-10 days and the pain increases, you should:
Consult a doctor for further examination, advice, or treatment.
If after 6-8 weeks and the pain increases, you should:
You may need to have an X-ray, MRI or blood test for further evaluation.
Treatment for Whiplash
If you suspect your pain is caused by whiplash, you should:
See a doctor to get your neck assessed to exclude more serious bone or nerve injury.
If after 7-10 days you are not able to resume normal activities, you should:
Consult a doctor for further examination, advice, or treatment.
If after 6-8 weeks you are not recovering as expected, you should:
See a specialist regarding the benefit from facet joint injections.
You may need to have an X-ray, MRI or blood test for further evaluation.
psNeck and BackComments Off on Discogenic Back Pain Specialist
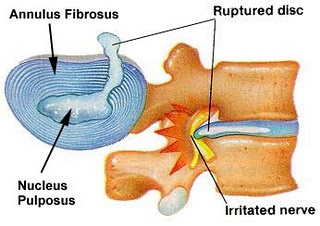
When the annulus – the cover around the disc – tears, pain may occur. The annulus has nerve fibres, unlike the nucleus. When a tear occurs in the annulus, you may feel pain in the neck or lower back and areas overlying and around the tear. Pain may also travel down the arm or leg as with a true disc herniation.
Although an annular tear may produce pain that is referred or travels from the neck to an arm or from the lower back to a leg, it can never produce weakness or numbness. Only compression of the root can do that. Annular tears usually heal inn two to three months. However, they can tear again and cause pain again. This phenomenon is part of chronic discogenic pain. Discogenic pain, to the extent it is understood arises from abnormalities within the disc itself and has nothing to do with pain from a herniation, which occurs as a result of root compression by herniated disc.
Diagnosing Discogenic Pain
If an MRI shows a tear in the annulus or disc covering, usually coupled with other signs of disc degeneration.
Conservative Treatment of Discogenic Pain
Most people with annular tears recover with rest, pain medications, and a gradual resumption of normal activity. NSAIDs, muscle relaxants for spasm, and narcotics should be used as needed. Sometimes physiotherapy or epidural steroid injections may be used.
Most discogenic pain comes from an annular tear, although that may not be the whole story. Although there is no pressure on a spinal root in this condition, it does hurt. Activity reduction and lifestyle modification so as not to bear down – risking a further tear or a disc herniation through the tear – is important.
The vast majority of annular tears causing discogenic pain heal without difficulty. For those that don’t, there are several minimally interventional treatments presented below.
Epidural Steroid Injections
Besides acting on the swollen, inflamed nerves, the liquid in the steroid epidural injection also flushes away the chemicals produced by the annular tears that cause root inflammation and pain. Studies on epidurals show that they work well for a very small specific group of people, such as those under forty who have not previously has surgery or those with pain lasting less than three months. If used at all, epidural injections are most appropriate as a short-term treatment for those whose spine-related pain also travels or radiates down a leg or arm.
Key Points about Discogenic Back Pain
Discogenic back pain arises from abnormalities within the disc itself. It has nothing to do with pain from a herniation, which occurs as a result of root decompression by the herniated disc.
Most people with discogenic back pain recover with rest, pain-relieving medications, and other conservative treatment.
Epidural injections work well for short-term relief on some people with this type of pain.
There is no need surgery for most discogenic back pain.
psNeck and Back,SpineComments Off on Pain from Spinal Disc Herniation Specialist
As we age and our spinal discs begin to dry out, shrink, and become less stable, they can herniate, lose their covering, press on a nerve, and cause all manner of trouble. A herniated disc is an extrusion of a piece of nucleus (the gel-like center) through a tear in the annulus (the tough, leatherlike outer cover). Most disc ruptures occur between ages thirty and forty; the discs still contain a normal amount of gel, but the annulus is beginning to wear out. If the gel remains inside the cover, it is a disc protrusion. If it escapes through a torn annulus, it is a disc extrusion. Extruded pieces of disc may move up or down the spinal canal a quarter to a half-inch or so from the area of herniation. Discs may protrude to the front, the sides, or to the back.
Most disc herniations occur in areas where the spine is maximally bent forward. The forward bending of these segments results in the vertebral bodies coming closer together toward the spinal canal than in the front of the spine. This places more stress on that part of the annulus and disc facing the spinal canal. The lower neck and the lowermost lumbar spine cause the most problems. Lumbar discs are herniated several times more frequently that their cervical counterparts. Presumably, this is because of greater weight on the lumbar spine. Thoracic herniations are rare; those causing problems are even less frequent. Disc herniations may be preceded by a history of intermittent episodes of back or neck pain, possibly with twinges in the leg or arm. This is from the annulus;s being stretched and under tension. After the disc fully herniates, the pain increases and is usually accompanied by pain radiating down the leg or arm, depending on which root or roots are irritated.
If a herniated disc does compress a nerve root, it can cause not only pain but also possible weakness, numbness, and loss of normal reflexes in the area supplied by the root. Cervical or thoracic-herniated discs can compress the spinal cord, and the large lumbar discs can significantly compress the cauda equina. These herniations can result in arm or leg weakness, numbness below the area of the cord or cauda equina compressed by the disc, and bowel and bladder disturbance. Significant compression of the cauda equina usually also causes severe pain in both legs. Depending on the extent of deficit caused by this type of herniation, emergency neurosurgical decompression my be required to minimise the damage to the nervous system and prevent the creation of permanent nerve damage.
Disc herniations are common; 70 percent to 80 percent improve with time and care. Some herniate and heal, then herniate and heal again. Too often, however, people rush to have unnecessary surgery. They then may spend the rest of their lives repairing the repair.
Cervical Discs
Cervical-disc herniations are less common than lumbar disc herniations even though you move your neck more often than you do your lower back. There is substantially less weight in the neck than in the lumbar area. Nevertheless, because the cervical spine has a smaller internal diameter – canal – and smaller foramen than other parts of the spine, small herniations are more likely to impinge on a spinal root and cause pain to radiate down the arm. Numbing and tingling may occur a far down as the fingertips. The pain is usually most severe when the disc first herniates and compresses the root. A cervical-disc herniation into the canal can also damage the spinal cord.
Herniation of the C4-5 disc can affect the C5 nerve root. This causes pain in the neck and over to the side of the shoulder and weakness in the other shoulder muscles and in the muscle that bends the elbow. The biceps reflex may be reduced. Sensory changes, such as numbness and tingling, may also occur in the deltoid area, on the side of the shoulder.
Herniation of the C5-6 disc affects the C6 root. This can cause pain running from the neck down the arm and hand to the thumb and forefinger. Weakness of some shoulder muscles, the biceps, and the wrist muscles that bend the wrists down and to the inside may exist. Sensory changes, along with pain, may extend to the lower arm and the thumb side of the hand. The biceps reflex may be reduced. This is one of the most common results of a cerivcal disc herniation.
Herniation of C6-7 disc affects the C7 root. Like the previous level, this is also a common site of disc herniation. Pain may radiate down to deep in the forearm and into the middle finger, and sensory changes may occur in the same area. Damage to this root causes weakness in the muscle that bends the wrist down and inward, other muscles that bend the wrist downward, and those that bend the finger, the triceps, and the muscles that raise the wrist inward, and some muscles that straighten the fingers. The triceps reflex may be reduced.
Herniation of the C7-T1 disc affects the C8 root. Pain may radiate down along the small-finger side of the arm and terminate in the little finger. Sensory changes may occur in the same area. Damage to this root causes weakness in the triceps, the muscles that raise and bend the wrist and fingers, and those that allow you to spread apart and bring together your fingers. The triceps reflex may be reduced.
These are typical but not absolute pain patterns. The same applies to the lumbar roots described below. Some people are wired a little differently.
Arm pain from a herniated cervical disc is common, usually occurring in thirty- to fifty-year-olds. Unlike lumbar discs, which usually herniate from lifting, carrying, or excessive bending, cervical discs are often herniated while we sleep.
Turning the head from side to side or sleeping on the stomach with the head turned to the side is a good position to herniate an already weakened cervical disc. This change in position in bed often occurs as we enter and leave the state of dream sleep. So we may awaken with a crick in our neck, which travels down an arm. Cervical-disc herniations may produce worse pain when a person carries or lifts on the side of the herniation, turns the head to the side, or strains ot bears down through lifting a heavy load, coughing, sneezing, or having a bowel movement.
Bearing down makes all disc herniation pain at any spinal level worse because the pressure within the chest and abdomen increases during this type of effort and is transmitted to the inside of the discs. Any weakness within the annulus allows more disc material to herniate during increased pressure within the disc. In turn, more pressure may be exerted on a compromised spinal root, causing more pain.
Pain from cervical and lumbar herniations is typically reduced when you bend forward, thus opening the spinal canal and the foramina and thereby relieving the pressure on the root. Pain is worse when you bend forward, thus opening the spinal canal and the foramina and thereby relieving the pressure on the root. Pain is worse when you bend backward. In any disc herniation causing root compression, you may experience throbbing pain like a toothache, pins and needles, or burning sensation. The pain may be so severe that your back is locked in spasm, or it may be just a dull ache that increases with movement.
Thoracic Discs
The thoracic spine, behind the chest, is relatively safe from disc herniation because it hardly moves and is curved slightly backward, thus placing more pressure on the front of the discs. When these discs herniate, it is due to the weight on the thoracic spine from the body above the level of herniation or from a trauma, such as falling. A thoracic-disc herniation may cause pain radiating under the ribs, in the chest, upper abdomen, or around the thoracic spine and shoulder blades in the back of the body. Symptoms vary from a band of chest pain , deep, dull pain behind the breastplate or stomach, or pain between the shoulder blades. Disc herniations of this type are not easily recognised by nonspecialists unfamiliar with this problem.
Lumbar Discs
Any lumbar disc can rupture. The ones at the bottom of the spine herniate most frequently because they carry a greater proportion of the body’s weight. Herniated lumbar discs can often be identified by the pattern of pain and nerve loss in the leg. The spinal cord does not extend below L1-2. However, disc herniation in the lumbar spine that primarily affects the foramen – herniating off to the side of the spine – usually damages the exiting root at that level. Those that herniate centrally into the canal may damage the root that exits the spine one level below. This depends on the size of the canal in relation to the disc and the location of the herniation and the roots exiting the dural sac.
At the L3-4 level, a disc herniation may result in damage to the L3 root exiting the spine, on the side of the disc, in the foramen, or the L4 root off to one side in the canal. The same pattern applies to the other lumbar discs. The following patterns of pain, weakness, numbness, and reflex loss exist for various lumbar roots likely to be affected by disc herniations.
Damage to the L3 root results in pain to the front of the thigh to the inner part of the knee. Sensory changes, such as numbness and tingling, may occur in this area. Weakness may occur in the quadriceps and the muscle that raises the thigh with the knee bent and the foot on the ground. There may be reduction of the knee reflex.
If the L4 root is damaged, it may result in pain along the nerve root that runs down the leg to the front of the ankle. Sensory changes may occur in the same area. Weakness of the quadriceps and reduction of the knee reflex may exist.
The L5 root, if damaged, results in pain that radiates down the leg, over the outside of the calf, and over the arch of the foot to the big toe. Muscles controlled by this root raise the foot and curl the big toe upward. Sensory changes may occur in the same area. There is no reflex loss with damage to this root.
The S1 nerve root can also be damaged, usually from a disc herniation at L5-S1. This causes pain that radiates down the leg into the back of the calf and the outside of the foot. This root, if damaged, causes weakness of the muscle that allows you to stand on your toes. Sensation may be altered in the same area as the pain. The ankle reflex may be reduced.
Sciatica Pain from Lumbar Discs
Sciatica is a term used to describe pain radiating along the route of the sciatic nerve. Sciatica from disc herniations occurs most commonly from a lumbar disc pressing on the L4, L5, and S1 roots, all of which when compressed may radiate pain to the lower leg and foot. The sciatic nerve consists of the L5, S1, and S2 roots.
Generally, leg pain from lumbar-disc herniations is worse when sitting and possibly standing and walking and less when lying in bed on the back with a pillow under the knees or, possibly, on the side.
Diagnosing Nerve Pain From Disc Herniation
An MRI can obtain images from inside the spinal canal and is the most sensitive test for identifying the location of a disc herniation and nerve compression.
If you cannot have an MRI because of metal implant in your body, a CT scan can be done.
Conservative Treatment
Most people with herniated disc recover with rest and pain medications.
Medications
Anti-inflammatories, muscle relaxants or NSAIDs to reduce the inflammation around the root.
Epidurals
Epidurals are corticosteroids, combined with local anaesthetics, that are injected into the epidural space. It can help to reduce pain from root compression from disc herniations.
Treating Pain from Cervical-Disc Herniations
Most of the time, the pain from a herniated cervical disc can be controlled with medication and nonsurgical treatment. Wearing a soft cervical support collar for several weeks day and night helps rest your neck. However, wearing too long may weaken your neck muscles. Seek medical advice about long-term use.
Physiotherapy
Physiotherapy can help open up the cervical foramen where the nerve root exits the spinal canal.
Treating Pain from Lumbar-Disc Herniations
Relief from pain caused by lumbar-disc herniation calls for conservative treatment, such as medications and physiotherapy. You should get out of bed and ambulate as well as you can. Strict bed rest is not beneficial.
Surgery for Disc Herniation
Discectomy, in the neck, antterior decompression are all operations may be used to treat problems from a disc’s pressing a nerve root.
Surgery is sometimes indicated to decompress a root pressed between a disc and a piece of bone or ligament or to remove the portion of the disc that is pressing on the nerve.
Certain types of muscle weakness may lead to early surgery. If your foot is in a dropped position and cannot be raised off the floor, early surgical intervention must be considered.
Surgery does help to eliminate the symptoms of sciatica more quickly than conservative – nonsurgical – treatment.
Key Points about Back Pain from Disc Herniations
Most disc herniations occur at spinal segments that are maximally bent foward: the lower neck and lumbar spine.
A lower lumbar-disc herniation may cause true nerve root pain, called sciatica.
An MRI can obtain images from inside the spinal canal and foramen and is the most sensitive test for identifying the location of a disc herniation and nerve compression.
Most people with herninated disc recover with rest, pain medications, and, sometimes physiotherapy or epidural injections.
Progressive or sudden onset of neurological problems or bowel or bladder problems may require surgical intervention.
Whiplash is the rapid bending forward and extension backward of the spine, usually the cervical spine, by an abrupt change in the speed and direction in which you are in is obviously traveling faster that yours. When the collision occurs, your car is projected forward, forcing your head backward. Then you car rapidly decelerates, hits another car ahead of you, or you slam on the brakes to avoid it, and your head is thrown forward. All this may occur within seconds and cause damage to the facets and their coverings, discs, and the muscles around and the ligaments supporting the spine.
The whiplash may also cause the brain to bounce back and forth inside the skull. The brain is a mass of nerve and other cells and blood vessels. It has the consistency of moderately firm butter and is supported by leatherlike sheets (dura) and surrounded by a leatherlike sac filled with spinal fluid. At the base of the brain, delicate nerves, a fraction of an inch in diameter, leave the buttery mass, enter holes in the skull, then can travel to your nose, eyes, ears, and other structures. You can readily understand that as a result of severe whiplash, in which the brain is thrown back and forth inside the dural sac inside the skull, damage to it and the nerves leaving it may occur. A whiplash injury may cause a mild concussion, which can affect thinking and mood. Double vision, ringing in the ears, and headaches are common. If the speed at which this accident occurs is high enough, broken vertebrae, a damaged spinal cord, and severe concussion or even a contusion or bruise of the brain, resulting in bleeding within it, can result. There are usually no broken bones, disc herniations, large blood clots, ripped muscle, or torn skin. The result of a whiplash injury is obviously painful, and the painful aftereffects, for unclear reasons, last varying times in different people.
Acute whiplash pain may cause local or widespread muscle spasm. For those with chronic pain, the facets are the usual culprits, although muscle spasm may still exist. The top three segments of facets, C2-3, C3-4, and C4-5, are responsible for head and upper neck pain. Lower facets may cause mid-to-lower neck, thoracic, and lumbar pain.
Whiplash injury may also cause what we call discogenic pain. Even when not herniated, discs may have a torn covering (annulus) and internal tears within the nucleus. The torn annulus can be seen on MRIs. Not all discs with a torn annulus are painful. The C2-3 and C3-4 discs may cause headache and these and the C4-5 discs may also cause upper neck pain. Like facets, lower discs may cause lower neck, thoracic, or lumbar pain. Discogenic and facet pain may coexist.
Symptoms of Whiplash
Symptoms may occur right after the injury or may be delayed for several days. They include:
neck pain and stiffness
headaches
pain in the shoulder or between the shoulder blades
pain, numbness, or tingling (paresthesia) in he arm and/or hand
less commonly, low-back pain, with possible radiation into the buttocks, groin, hips, and thighs
Treating Cervical Whiplash Pain
Most whiplash-caused head and neck pain goes away in a few weeks to a few months. In the past, whiplash was often treated by immobilising the neck in a cervical collar; today, we encourage early movement rather than keeping the neck rigid. The collar is the best used intermittently for short periods.
In the first twenty-four hours after injury, apply heat and keep moving the neck slowly and gently. No single treatment has proven effective, but exercises, physiotherapy, cervical collars, medication, and injections have all helped some people some of the time.
Key Points about Whiplash
Whiplash is one of the most controversial conditions in medicine.
It is most frequently caused by a rear-end auto accident.
Most whiplash heals in a matter of weeks, but 20 percent to 40 percent persist for years.
It can lead to chronic neck, back, and head pain.
Cervical facets and muscle spasm cause the pain.
Whiplash can also cause discogenic pain.
Because it is test-negative, others frequently don’t believe that you have it.
Diagnosis must be done by ruling out all other possibilities.
It is treated with medication, physiotherapy and injection.
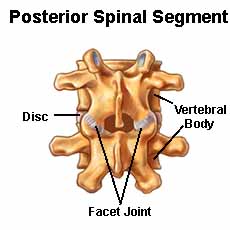
Many people are unaware that they have joints in their spine. There are two tiny facets one on each side of each vertebra to keep the spine stable. As do the shoulder and the knee, spinal facets joint two bones: the vertebra above and below. Spinal facets are true synovial joints. They have a capsule (synovium) that is lubricated by fluid and are filled by a network of pain-sensitive nerve fibres. These small, delicate joints are prone to injury, deterioration, and, in some diseases, inflammation, and they sometimes become sources of chronic neck and back pain independent of the discs and spinal nerves. After muscle pain, facet pain is probably the most common cause of low-back pain.
Lumbar-facet Pain
Lumbar-facet pain is the most common (though facet pain can occur in any part of the back). The telling sign of lumbar-facet pain is black and possibly buttock, groin, and thigh pain, especially while sitting or arching your back, which increases the pressure on the facets in the back of the spine. Bending forward or lying down usually relieves lumbar-facet pain.
Cervical-facet Pain
Cervical-facet pain is the second most common facet problem and may cause headaches, shoulder, and occasionally arm pain. These facets are often more painful when the neck is bent backward or to the sides, which increases pressure on the facets. Headache from facet pain (cervicogenic headache) occurs in the morning after a night tossing and turning, which also increases pressure on these joints.
Thoracic-facet Pain
Thoracic-facet pain is less common. These joints become injured when excessive amounts of rotation and extension cause a sharp pain anywhere between the upper shoulder blade and the area over the lower ribs. Pain from thoracic facets doesn’t usually travel to the side or front of the chest. Thoracic vertebrae form a relatively immobile segment of the spine compared to the highly mobile neck and lumbar area. Therefore, the thoracic discs and facets are less likely to wear out.
How Facet Pain Develops
The vertebral bodies, separated by the discs, make up the front of the spine and carry the weight of the structure. As the discs degenerate, the facets end up carrying more weight than they should, leading them to wear down and become painful. When facets wear out they can become arthritic, just as occurs in other joints, such as the knees, hips, or fingers.
Osteoarthritis usually develops in the facets of the neck and lower back. The synovium wears out, bone surfaces rub together, and the facets become painful. With time, calcified outgrowths, called osteophytes, develop around the facets, degenerated discs, and supporting ligaments of the spine. The result is loss of flexibility and possibly pain.
Being overweight is an increasingly common cause of problems with lumbar facets. Heavy people wear down their discs earlier and therefore may develop chronic facet pain – among other spinal problems – early in their lives.
Facets can be injured from trauma, such as whiplash from a rear-end auto collision. They can also be injured in sports, such as by being tackled in football or falling off a horse. Golfers are prime candidates for lumbar and thoracic facet injury because of the repetitive twisting motions as they swing the club. A sudden excessive movement – especially backward or to the side – can traumatise the joint and cause pain that can last several days. Sometimes this pain becomes chronic, for reasons that are poorly understood
Spondylolisthesis or slippage of one vertebra over another can also cause low back pain from the facets and other structures. Pain can be controlled by treating the facets only if the slippage is of a low degree and the spine is relatively stable. If the vertebrae wiggle significantly, facet treatment won’t be enough. Medication and lifestyle modification may help you to tolerate your back pain; if they don’t, surgery – fusion – is needed to stabilise your spine.
Diagnosing Facet Pain
Facet problems are identified by the pattern of referred pain, local tenderness over the site, and pain in certain body positions. Your doctor will try to find the pain by poking or moving the suspected painful areas during a physical exam. Physical examination should reveal tenderness over the affected facets and possibly painful trigger points in overlying or nearby muscles and in one-sided lumbar pain, possibly pain in the sacroiliac joint and bursa overlying the hip on the same side as the painful facets.
To make the diagnosis of the facet pain and accompanying myofascial or other test-negative pain and to exclude other possible anatomically based causes of pain, it may be necessary to have a MRI of the painful areas of the spine, and possibly, of the painful pelvis and hip.
Chronic facet pain may come from long-term changes in the joint, detectable by radiological studies, even though facet pain itself is not. Normal appearing facets may hurt, and those that appear arthritic may not. Therefore, facet pain is a test-negative condition, one whose diagnosis is made clinically (using history and examination), not by radiological or other conventional studies.
Treating Facet Pain
An acute episode of facet pain can be treated with rest, medicines or physiotherapist.
You may need injections of local anaesthetics and corticosteroids into any especially painful muscles with trigger points (myofascial pain) associated with the facet problem. If relevant, the bursa overlying the hip may also be injected before starting to exercise. This needed exercise may be painful for the first few weeks.
Treatment of Chronic Facet Pain with Injections
Diagnosis and preliminary treatment of chronic facet-related pain can be done by injections into the facets or the nerves supplying these joints. Just as epidural injections are used to treat root pain within the spinal column, facet-joint injections are sometimes used to diagnose and, for the short term, treat pain from the facet joints. If the facets are in fact the sole or a major cause of pain, injections of anti-inflammatory corticosteroids and local anaesthetics directly into the joints or over the nerves transmitting pain impulses from the facets to the spinal cord may reduce pain and facilitate the rehabilitative therapy.
The injection of anaesthetic briefly blocks the pain signals emanating from the joint, and the corticosteroid reduces any inflammation of the joint and surrounding structures.
Key Points about Facet Pain
Facet are small joints, one on each side in the back of the spine, that connect two vertebrae.
Facets keep your spine stable but are not made to bear considerable weight.
Facets forced to bear weight as the discs degenerate are prone to degeneration.
After muscle spasm, facet pain is probably the most common cause of low-back pain.
Facet pain can occur anywhere in the spine.
It is most common in the lower back.
Facets that appear normal on radiologic studies may hurt, while those that appear arthritis may not.
Osteoarthritis can develop in the facets of the neck and lower back.
Being overweight causes problems with lumbar facets sooner rather than later.