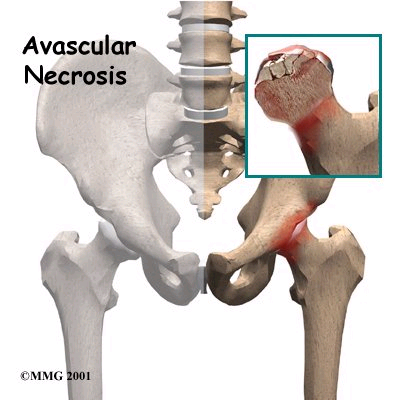
Avascular necrosis (AVN) or osteonecrosis is a disease where the blood flow to the femoral head is damaged. Part of the bone of the femoral head then undergoes necrosis – it dies. When the bone dies, it becomes painful. The pain may be present either with activity or at rest. The joint surface of the femoral head may collapse and arthritis will result.
Symptoms usually present twelve to eighteen months after the initial damage to the bone. The cause of AVN may be traumatic such as dislocation or femoral neck fracture, or may be atraumatic and systemic.
When the cause is traumatic, a fracture disrupts the blood supply to the femoral head. Blood vessels run through the posterior capsule of the hip joint which is injured by the fracture. The blood supply to the femoral head is interrupted and AVN develops. A similar mechanism happens with traumatic dislocation. The head of the femur is forced out of the socket and the capsule is torn. Most often dislocation occurs in a posterior discretion.
Some studies show that the time from when the hip is dislocated to when it is put back in place is a factor in whether AVN develops. The shorter the time the better. AVN may develop following a femoral neck fracture even though the fracture itself heals.
Many systemic factors have been felt to lead to avascular necrosis. These include:
- Steroid therapy
- Alcoholism
- Collagen vascular disease
- Graucher’s disease
- Arterial occlusion
- Blood clotting disorders
- Other diseases of circulation
- Other blood diseases called haemoglobinopathies where small vessels in the head of the femur may be occluded.

Radiation injury and caisson, or dysbaric disease, are two other causes of AVN which do not fit the trauma or systemic categories. Radiation injury follows large doses of radiation given to a patient to treat other conditions. Caisson disease can occur in deep sea divers who return to the surface too quickly without allowing adequate time to decompress. With good training this rarely happens.
Patients who have had organ transplants are known to develop avascular necrosis, possibly because they medication to suppress their immune systems. In some cases, the cause of AVN may be idiopathic. This means that it develops spontaneously with no known cause.
Even though steroid therapy is one of the most common causes of AVN it is not known what dose of steroids or what length of treatment causes the disease. In systemic conditions, it is not clear if AVN occurs with a single insult to the circulation or gradually over time. It may be the result of multiple insults to the marrow in the same area.
The first symptom of avascular necrosis is pain. At the onset of the disease, the hip maintains a good range of motion. As the disease progresses, range of motion decreases. Examination and x-ray findings become similar to those in osteoarthritis. AVN is different from osteoarthritis, however, because disease first develops in the bone rather than in the joint.
On x-ray, AVN appears as a wedge of abnormal bone in the superior, or upper, part of the head of the femur. On a lateral x-ray a crescent sign may be visible. This is a clear line just below the surface of the joint. At this point the surface remains intact and has not collapsed. Within the femoral head an area of dense whitish appearing bone is visible. This indicated a process of bone repair called creeping substitution.
Often the diagnosis and surgical treatment of AVN are delayed. If pain is present and there are no changes on x-ray, the diagnosis may sometimes be made with an MRI study. Patients may delay treatment until symptoms are more severe. At the very least they should seek an orthopaedic consultation. If they wait too long, some of the more conservative options such as core decompression may no longer be helpful and hip replacement is required.
Hip replacement is not the only treatment option for avascular necrosis. If the disease is not far advanced, then other procedures may be done in an attempt to save the femoral head. This is particularly true for patients in their 30s and 40s. More conservative procedures include:
- Core decompression with or without bone grafting
- Bone grafting through a cortical window
- Osteotomy
- Resurfacing
Resurfacing may not be possible if there is too much bone collapse or there is involvement of the bone in the neck of the femur.
For older patients and for younger patients in whom the femoral head has collapsed, hip replacement is the surgical treatment of choice.

